Click on the links below.
Thyrotoxicosis affects ten times as many women as men; there are 3 cases per 1000 people.
Graves' disease, multinodular goitre and autonomously functioning nodules are common causes of thyrotoxicosis, with thyroid stimulating hormone adenomas (TSH-oma) and drug causes, e.g. amiodarone, less common.
Always consider the possibility of thyroid neoplasia in any patient with goitre.
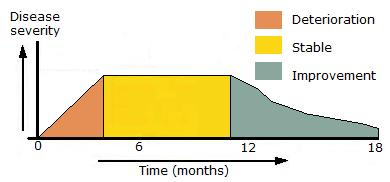
Thyroid eye disease runs a typical course (Fig 1) with lid lag and subsequent proptosis. It may be more pronounced if the patient smokes.
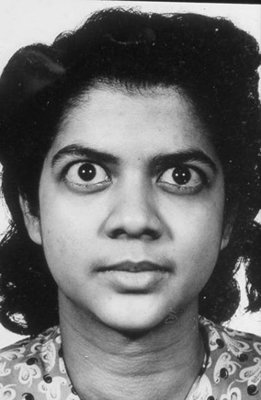
The most common cause in younger women is Graves' disease (Fig 2), where prevalence is up to 2% of the female population. Hyperthyroidism occurs in about 0.2-0.4% of all pregnancies.
Note: Biochemical results of thyroid function tests taken during hyperemesis gravidarum may suggest hyperthyroidism but may not require intervention, at least initially, as these abnormalities can resolve spontaneously.