Introduction
In biliary obstruction and/or sepsis where surgery and endoscopic retrograde cholangiopancreatography (ERCP) cannot be performed, percutaneous transhepatic cholangiography (PTC) may be indicated. The biliary tree is accessed via the anterior abdominal wall. However, advances in non-invasive imaging, in particular CT and magnetic resonance cholangiography, have markedly decreased the need for PTC in the investigation of these patients.
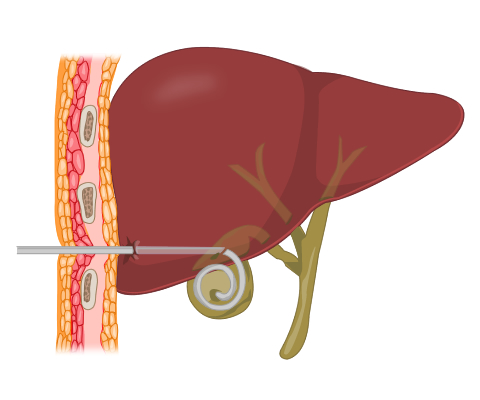
Much more common in contemporary practice is percutaneous cholecystostomy. The gallbladder is approached via the anterior abdominal wall (Fig 1). Drainage of biliary contents is maintained by leaving an indwelling catheter. This minimally invasive procedure can aid stabilisation of a patient to enable a more measured surgical approach with time for therapeutic planning.
Question: Which patients might benefit from PTC or cholecystostomy?
Click here for the answer.
In biliary obstruction and/or sepsis where surgery and endoscopic retrograde cholangiopancreatography (ERCP) cannot be performed, percutaneous transhepatic cholangiography (PTC) may be indicated. The biliary tree is accessed via the anterior abdominal wall. However, advances in non-invasive imaging, in particular CT and magnetic resonance cholangiography, have markedly decreased the need for PTC in the investigation of these patients.
Much more common in contemporary practice is percutaneous cholecystostomy. The gallbladder is approached via the anterior abdominal wall (Fig 1). Drainage of biliary contents is maintained by leaving an indwelling catheter. This minimally invasive procedure can aid stabilisation of a patient to enable a more measured surgical approach with time for therapeutic planning.
Question: Which patients might benefit from PTC or cholecystostomy?
Answer:
If any of the following apply to your patient, PTC could be of benefit:
- Do they have obstructive jaundice?
- Have previous attempts at ERCP failed?
- Are they unfit for ERCP?
- Do they have multiple co-morbidities?
- Do they have any difficulties swallowing?
If any of these apply, cholecystostomy may be appropriate:
- Does the patient have severe cholecystitis or gallbladder empyema?
- Are they unfit for laparoscopic cholecystectomy?
- Are they critically ill in ITU?
Click on the tabs above for more information, or Next to move on to a different procedure.
Patient Preparation
Feedback
Keyword matches are highlighted.
It is essential to:
- Review all available imaging to confirm the indication for the procedure. It also helps to assess gallbladder anatomy and establish safe access route to the gallbladder
- Check full blood count and coagulation profile to assess the risk of haemorrhage
- Obtain informed consent for the procedure
- Obtain good peripheral IV access
- Administer broad-spectrum IV antibiotics 1-4 hours prior to the procedure. Septic patients are often already on parenteral antibiotics
- Arrange analgesia and sedation according to patient comfort
Remember, patients with jaundice often have deranged liver function and abnormal clotting. Check platelets and coagulation before going ahead.
Technique
Using aseptic technique and following infiltration of local anaesthetic agent, a needle is passed into the right upper quadrant under ultrasound guidance. In PTC, the liver parenchyma must be crossed in order to cannulate the biliary tree. Cholecystostomy can be performed via the liver (which means peritoneal irritation will be avoided in the event of any subsequent bile leakage) but the gallbladder can be punctured directly after traversing the anterior abdominal wall.
A guidewire is used to exchange the needle for a dilator and an 8 French or larger pigtail drain is placed within the gallbladder (Fig 1). The drain can often be visualised under ultrasound.
Aspiration of bile/pus from the drain confirms satisfactory position. A sample from the aspirate is sent off to the laboratory for microbiological studies.
The catheter is left to drain freely under gravity. Some operators choose to actively aspirate all contents from the gallbladder and then leave the catheter on free drainage.
Due to portability and ease, this procedure is often performed using ultrasound guidance. Fluoroscopy in the IR suite or CT can also be used, depending on local expertise.

Image reproduced with permission from Brighton & Sussex Medical School