Presentation
A 60-year-old female is seen in clinic after having a persistent fever, cough and malaise for several weeks. She has also been experiencing increasing breathlessness with moderate exertion and has gone off her food with a 2-stone loss in weight. She was given a course of antibiotics by her GP which hasn’t helped her symptoms.
Her past medical history is otherwise unremarkable.
She has never smoked cigarettes and has not travelled abroad over the last few years. She doesn’t have any pets and previously worked as a school teacher.
She is currently not taking any medications, but recently finished a week’s course of amoxicillin and clarithromycin. She has no known allergies.
Click the CXR tab.

CXR
Question: The GP requested a chest x-ray (Fig 1). What is your interpretation of it?
Click here for the answer.

Question: The GP requested a chest x-ray (Fig 1). What is your interpretation of it?
Answer: The x-ray demonstrates areas of bilateral patchy consolidation, more prominent in the right lower zone.
Click the Examination tab.
Initial Inv
Before clicking on the links below, consider what you are looking for in carrying out these initial investigations.
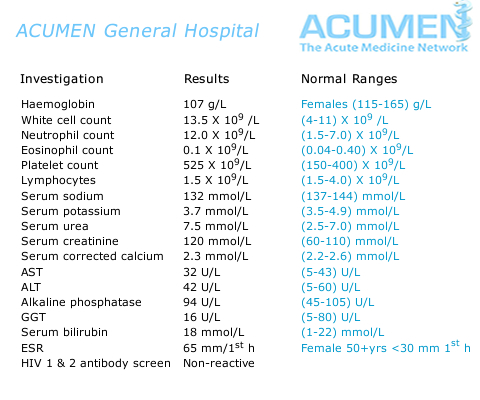
Blood tests (Fig 1)
Sputum culture (Fig 2)
Blood cultures (Fig 3)
Legionella/Pneumococcal urine antigen test (Fig 4)
ABG (Fig 5)
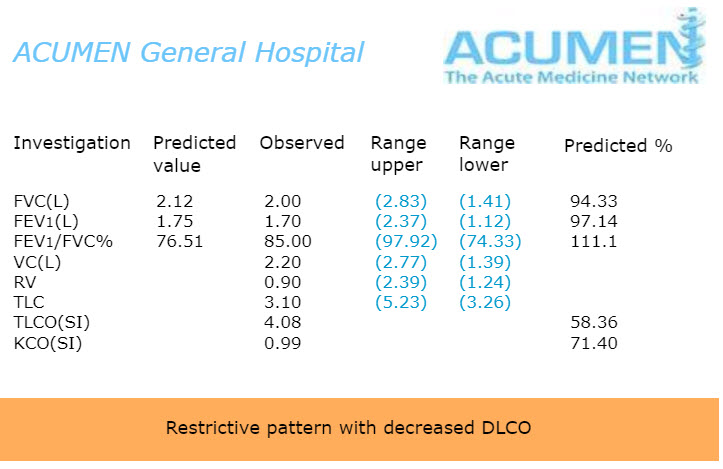
PFTs (Fig 6)
Click the HRCT tab when you are ready to move on.
HRCT
Click the links below.
Despite being treated with broad spectrum IV antibiotics and supplemental oxygen therapy for several days, the patient’s symptoms do not improve. A CT chest is requested.
Check both of the patient’s HRCT chest images, then compare your findings with the results below.
Click the Other Inv tab when you are ready to move on.
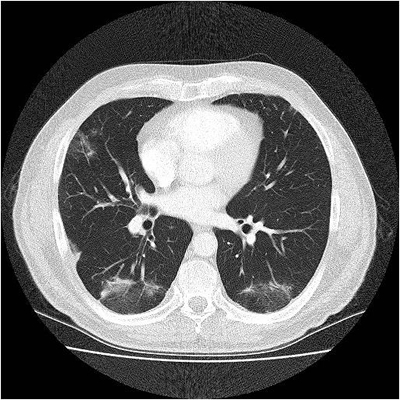
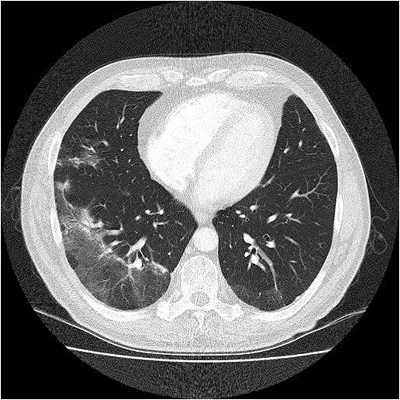
HRCT chest results
The images show multiple areas of bilateral patchy consolidation and ground glass opacification.
Which would be the most useful investigation(s) to obtain the diagnosis for this patient?
Select one or more options below.
Given the diagnosis, which of the following treatment options is the patient likely to respond to?
Select one option below.
Summary
COP is an organising pneumonia with no definite aetiology but has been associated with infections, malignancies and iatrogenic causes, i.e. medications and radiation [11].
Diagnosis requires excluding other possible causes as well as obtaining histology, ideally from a surgical lung biopsy. However, often these patients may be too ill to undergo such invasive procedures and may be given a trial of treatment without having obtained a histological diagnosis.
COP may respond well to corticosteroids with rapid improvement in the patient’s clinical condition. However, relapses are common after withdrawal of steroid therapy, and sometimes a longer duration of treatment is required [4].
Click Next to complete the session with a short Self Assessment.