Procedure
Click on the links below.
The primary role of endovascular coiling is to prevent rupture in unruptured aneurysms, and to prevent re-bleeding in ruptured aneurysms (Fig 1a). The use of detachable coils has become the preferred management option over neurosurgical clipping. The coils are pro-thrombotic and work to seal the aneurysm, thus reducing the pressure on its outer wall (Fig 1b).
Click on the tab at the top for more information, or Next to move on to a short Self Assessment.
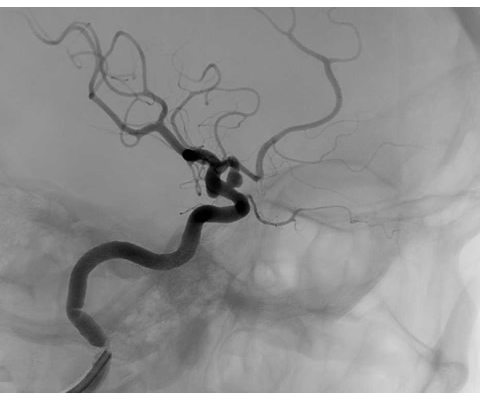
Fig 1a Aneurysm of the superior wall of the right internal carotid artery
Image reproduced with permission from Dr Panos Koumellis
Image reproduced with permission from Dr Panos Koumellis
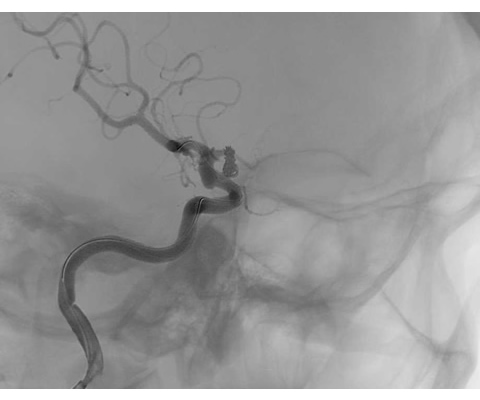
Fig 1b Post coiling appearances of the same patient
Image reproduced with permission from Dr Panos Koumellis
Image reproduced with permission from Dr Panos Koumellis
Indications
- Intracranial aneurysms
- Intracranial arteriovenous malformation (AVM) as part of a
multimodality approach:
- Pre-operative embolisation
- In conjunction with radiosurgery
- Curative embolisation
- Palliative embolisation for inoperable AVMs (controversial)
- Intracranial arteriovenous fistula (AVF)
- Bleeding intracranial vessel (usually when iatrogenic rather than post-traumatic)
- Intracranial vascular tumours (pre-operative or as palliative treatment for inoperable tumours)
Contraindications (relative)
- Prohibitive anatomy
- Significant atherosclerotic disease
- Life threatening contrast allergy
- Coagulation disorders or heparin hypersensitivity
- Bacteraemia
Preparation
- Record baseline neurological status
- Carry out pre-operative general anaesthetic risk assessment
- Give heparin before and during procedure
- Give aspirin in elective cases